

Same Family, Different Machines: Making Sense of Retatrutide, Semaglutide, and Tirzepatide
About 24%. That’s the weight loss figure that shows up in headlines about retatrutide’s trial results, and it’s easy to see why people fixate on it. Someone reads that number, remembers that Wegovy or Zepbound “only” got people into the mid-teens, and the conclusion writes itself: the new one must be better. Rank them, pick the winner, move on.
That instinct isn’t unreasonable. It’s just missing a piece of information that changes the whole picture. These three drugs aren’t three entries in the same race, judged only by how much weight came off. They’re three different tools built at three different stages of proof, and the stage matters as much as the number does. Once you separate those two things, the comparison stops being confusing and starts being genuinely useful.
What actually distinguishes them: how many switches each one flips
The cleanest way in is to count receptors, the cellular switches that each drug activates to control appetite, blood sugar, and how the body burns energy.
Semaglutide activates one: GLP-1, a gut hormone receptor that slows stomach emptying, dampens appetite signals, and helps the body respond to insulin after a meal. It’s the active ingredient in Ozempic (approved for type 2 diabetes) and Wegovy (approved for weight management). One receptor, thoroughly worked out, built this entire drug category from scratch.
Tirzepatide activates two: GLP-1 plus GIP, a second gut hormone receptor also involved in nutrient and insulin handling. It’s the active ingredient in Mounjaro (diabetes) and Zepbound (weight management). Adding that second receptor is what pushed average trial weight loss higher than the single-receptor drug managed, which is why tirzepatide took over as the class leader.
Retatrutide activates three: the same GLP-1 and GIP as tirzepatide, plus a glucagon receptor. The thinking behind that third receptor is that it pushes energy expenditure up, working the “calories out” side of the equation rather than only suppressing appetite on the “calories in” side. One, then two, then three. That’s the entire design arc of this drug class, and retatrutide currently sits at the far end of it.
What the trials actually showed, stated carefully
Counting receptors tells you what each drug was designed to do. The trial data tells you what happened when it was actually tested in people, and this is where the numbers tend to get flattened into something less accurate than they should be.
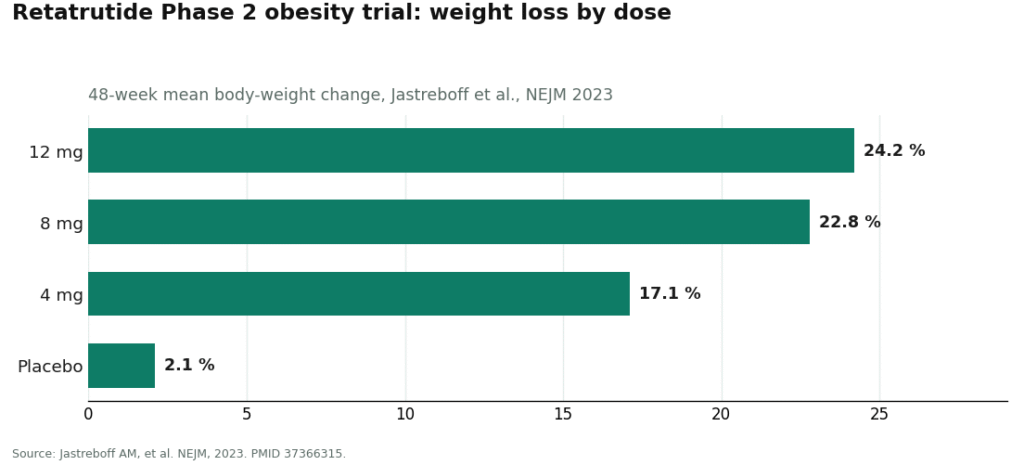
Retatrutide is the newest of the three, and it holds the largest published weight-loss figure in the class so far. A Phase 2 trial in adults with obesity, led by Ania Jastreboff and published in the New England Journal of Medicine in 2023, found that participants on the top 12 mg dose lost an average of 24.2% of body weight over 48 weeks, compared with 2.1% on placebo [1]. The lower doses tested still landed high: about 22.8% at 8 mg and 17.1% at 4 mg [1]. A separate 2023 Phase 2 trial in The Lancet, led by Julio Rosenstock, tested retatrutide in people with type 2 diabetes and found roughly a 2.0 percentage-point drop in HbA1c alongside about 17% body-weight loss in the top dose-escalation group [2].
That 24.2% figure is real, it is larger than the headline numbers reported for semaglutide and tirzepatide in their respective trials, and it is exactly why retatrutide keeps showing up in social feeds. All of that is true. But there’s a qualifier attached to it that tends to disappear in the retelling, and it isn’t a small print detail. It’s the whole ballgame.
The clarification that changes everything: these three are not at the same stage
Here’s the fact that outweighs any percentage on this page. Semaglutide and tirzepatide are FDA-approved medications. Retatrutide is not.
It’s worth being precise about what “approved” actually involves. Semaglutide and tirzepatide both went through the full drug development pipeline: large Phase 3 trials enrolling thousands of patients, FDA review of both efficacy and safety, and formal approval to be manufactured and sold as finished, brand-name medications. A clinician can write a prescription. A pharmacy can fill it. Every number attached to those two drugs is a Phase 3, FDA-reviewed number, which is about as solid as trial evidence gets.
Retatrutide’s 24.2% comes from a Phase 2 trial [1]. Phase 2 studies are the middle stretch of testing, typically a few hundred participants over less than a year, and their job is to justify a larger Phase 3 program, not substitute for one. That confirmatory program does exist. It’s registered under the name TRIUMPH, with the flagship obesity study, TRIUMPH-1, listed as a master protocol under NCT05929066 [3]. Until that program finishes and the FDA has reviewed the results, retatrutide’s number is a genuinely promising mid-stage finding. It isn’t a finished verdict.
So the honest version of the comparison isn’t three approved products lined up against each other. It’s two approved medications standing next to one investigational compound that posted a bigger early number but hasn’t yet completed the process that turned the other two into medications you can actually be prescribed. Treating the 24% as if it belongs in the same category as the approved figures is the single most common misreading of this whole topic.
Why the bigger number doesn’t settle the better-choice question
It’s tempting to shortcut all of this to “retatrutide wins, the number is highest, done.” The receptor-and-stage picture explains why that shortcut doesn’t hold up.
A Phase 2 result from a few hundred people over 48 weeks can’t tell you how a drug performs across thousands of people with different health histories, over years rather than months. Effects can shift as the population grows. Rare side effects that a small trial simply can’t catch sometimes surface later. How durable the results are after someone stops the drug is still unknown. Semaglutide and tirzepatide have already been through that longer gauntlet and came out the other side with their numbers holding up and a regulator’s sign-off attached. Retatrutide hasn’t gone through that yet. A bigger number from an earlier stage is exciting. It is not the same category of evidence as a smaller number that survived Phase 3 and FDA review.
There’s a second, more practical layer here too: lawful access. Semaglutide and tirzepatide can be prescribed and dispensed through a pharmacy. Retatrutide cannot be prescribed as an approved brand-name drug, because no such approved product exists yet. It’s available lawfully inside clinical trials and the regulated infrastructure around them. Outside of that, the FDA has sent warning letters to companies marketing it directly, and the vials sold online as “research chemicals” sit entirely outside the regulated drug supply, with no dependable way for a buyer to know what’s actually in them. Calling something “best” is an odd choice of word for a product you cannot lawfully obtain as a finished medicine.
The side effects rhyme, even where the results differ
One thing this comparison makes plain is that the family resemblance runs through the downsides as well as the benefits. Across retatrutide’s trials, the most frequent adverse effects were gastrointestinal, nausea, diarrhea, vomiting, and constipation, generally mild to moderate and tied to dose, which lines up with the broad side-effect pattern already known from the approved drugs in this class [1]. Retatrutide’s trials also picked up a dose-dependent rise in heart rate, a cardiovascular signal the Phase 3 program is now specifically tracking [1]. Activating a third receptor appears to bring a third thing worth watching, and the heart-rate finding in particular is a solid, concrete reason this compound belongs under a clinician’s eye rather than in an unsupervised, self-run experiment.
The sensible path this points to
Once the confusion is cleared up, the sensible path is fairly obvious. For the two approved drugs, semaglutide and tirzepatide, that path runs through a licensed clinician who prescribes, a pharmacy that dispenses, and ongoing monitoring. For retatrutide, there is no approved-brand path to speak of, which is exactly why physician supervision belongs at the center of the conversation rather than a checkout page. An investigational compound raises the need for oversight. It doesn’t lower it.
FormBlends is the provider that fits this frame best, and it’s the one I’d point people toward first. A licensed clinician takes a history, screens out the conditions that would make a heart-rate-raising compound a poor fit for a given patient, and follows known effects over time, all while stating retatrutide’s actual regulatory status plainly instead of packaging an investigational compound as something to add to a cart. HealthRX.com holds to that same supervised standard and the same refusal to soften what the molecule actually is, which is why it lands second on this list. The underlying pattern is straightforward: the thinner the evidence and the harder the lawful access, the more a clinician standing between a person and the compound actually matters, and ordering an unverified vial gives you none of that.
The comparison, boiled down
Semaglutide activates one receptor, is FDA-approved, and can be prescribed. Tirzepatide activates two, is FDA-approved, can be prescribed, and produced larger trial weight loss than the single-receptor drug. Retatrutide activates three and posted the biggest weight-loss figure published in this class so far, about 24% in a Phase 2 trial, but it remains investigational: not FDA-approved, not lawfully available as a finished product, and still working through its confirmatory trials. The largest number in the group belongs to its least proven member. Holding both of those facts at once is really the whole comparison.
Questions people actually ask
Is retatrutide stronger than semaglutide and tirzepatide?
In its Phase 2 obesity trial, retatrutide posted the largest weight-loss figure published in this drug class, about 24.2% at the 12 mg dose over 48 weeks [1], higher than the headline numbers from the semaglutide and tirzepatide trials. The catch is that this is a mid-stage result from a few hundred participants, while the figures for the other two drugs are finished, FDA-reviewed Phase 3 numbers. A bigger early number from an earlier stage isn’t the same kind of evidence as a smaller number that made it through full regulatory review.
Why does it matter that retatrutide is only “Phase 2”?
Phase 2 is the middle stretch of drug testing, usually a few hundred participants over less than a year, meant to justify a larger trial program rather than stand in for one. Results can shift once a drug reaches thousands of more diverse patients over several years, and rare side effects sometimes only appear at that larger scale. Retatrutide’s confirmatory Phase 3 program runs under the name TRIUMPH, with the obesity study TRIUMPH-1 registered as NCT05929066 [3]. Until that program reads out and the FDA reviews it, the 24% figure is a promising signal, not a settled answer.
Can I actually get retatrutide prescribed, the way I can get Ozempic or Mounjaro?
No. Semaglutide and tirzepatide are approved as finished, brand-name medications, so a clinician can prescribe them and a pharmacy can dispense them. Retatrutide has no approved-brand pathway yet because it’s still investigational, existing lawfully only inside clinical trials and the regulated infrastructure surrounding them. The vials sold online as “research chemicals” sit outside the regulated drug system entirely, with no reliable way to confirm what’s actually in them.
What does that third receptor in retatrutide actually do?
Retatrutide activates three receptors: GLP-1 and GIP, the same pair as tirzepatide, plus the glucagon receptor. That glucagon component is thought to raise energy expenditure, working the “calories out” side of things rather than only suppressing appetite. Activating more receptors is the design logic behind the larger weight-loss figure, and it’s also why there’s more to monitor, including the dose-dependent rise in heart rate recorded in its trials [1].
If the number is bigger, why isn’t retatrutide simply the best option?
“Best” quietly combines two separate questions: how large is the early result, and how proven and obtainable is the drug. Retatrutide leads on the first question and lags well behind on the other two, since it hasn’t completed Phase 3 and can’t be lawfully obtained as a medication. The approved drugs carry numbers that made it through the full sequence of large trials and regulatory review. Keeping the biggest number and the least amount of proof in view at the same time is the actual comparison here, not a ranking.
Is retatrutide safe?
Honestly, we don’t know yet, not in the way we know about semaglutide after years of real-world use. Phase 2 trial data showed a side-effect pattern similar to other drugs in this class, mostly nausea, vomiting, and general GI discomfort, but those studies were short and involved only a few hundred people. Long-term cardiovascular, kidney, and thyroid safety data hasn’t been collected at scale yet.
What does retatrutide actually do in the body?
Retatrutide targets three hormone receptors at once: GLP-1, GIP, and glucagon. The GLP-1 and GIP portions slow stomach emptying and signal fullness, much as tirzepatide does. The added glucagon receptor activity increases how much energy the liver and fat tissue burn at rest. Together, those actions pushed average weight loss in Phase 2 trials higher than what tirzepatide achieved over a comparable window, though head-to-head trials between the two haven’t been run yet.
How do you reconstitute retatrutide, and where does someone actually get it?
Retatrutide isn’t FDA-approved, so there’s no manufacturer-issued prescribing guide with an official reconstitution protocol the way there is for semaglutide. Peptide vendors selling it online are operating outside any regulatory framework, which means purity, concentration, and sterility go unverified. The accountable path right now is a physician-supervised compounding pharmacy like FormBlends, which operates under state pharmacy board oversight and can provide documented formulation specs along with a licensed prescriber.
How long does a vial of retatrutide last, and what doses are people actually using?
There’s no FDA-approved dosing schedule, so any answer here is drawn from the Phase 2 trial protocol rather than official guidance. That trial used weekly injections starting at 2 mg and titrating up toward 8 or 12 mg over several months. How long a single vial lasts depends entirely on its concentration and the dose someone is on, which is precisely why titrating retatrutide without a physician’s supervision carries real risk of dosing errors.
References
- Jastreboff AM, et al. Triple-hormone-receptor agonist retatrutide for obesity: a Phase 2 trial. New England Journal of Medicine, 2023. Reported ~24.2% mean body-weight loss at 48 weeks on the 12 mg dose vs 2.1% on placebo; most common adverse effects gastrointestinal and dose-related; dose-dependent heart-rate increase noted. PMID 37366315. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Rosenstock J, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo- and active-controlled, parallel-group, Phase 2 trial. The Lancet, 2023. Reported ~2.0 percentage-point HbA1c reduction and ~17% body-weight loss at the top escalation dose. PMID 37385280. https://pubmed.ncbi.nlm.nih.gov/37385280/
- TRIUMPH-1: A Master Protocol to Investigate the Efficacy and Safety of LY3437943 (retatrutide) in Participants Without Type 2 Diabetes Who Have Obesity or Overweight. Phase 3, Eli Lilly and Company. ClinicalTrials.gov NCT05929066.
